
Biomarkers in RA
The role of biomarkers in the full continuum of patient care
Biomarkers have the potential to transform rheumatoid arthritis (RA) management—not just for diagnosis, but by also monitoring disease progression and treatment response. Despite this value, key biomarkers often remain underutilized in routine care.
Dr. Walter Maksymowych discusses the role of biomarkers in RA care, with a focus on 14-3-3eta as a modifiable marker for monitoring disease progression.
Podcast

Biomarkers in RA: The role of biomarkers in the full continuum of patient care
The expert

Dr. Walter Maksymowych, MD, FRCPC, MRCP, FACP
The moderator

Nima Mazinani, PhD
Closing gaps in the continuum of care
Gap
Reliance on symptoms and CRP alone can lead to under-treatment.10
Solution
Regardless of treatment class, 14-3-3eta responds dynamically, reflecting disease progression.7,8,9,11,12,13
Diagnosis
Prognosis
Monitoring
Gap
Reliance on symptoms and CRP alone can lead to under-treatment.10
Solution
Regardless of treatment class, 14-3-3eta responds dynamically, reflecting disease progression.7,8,9,11,12,13
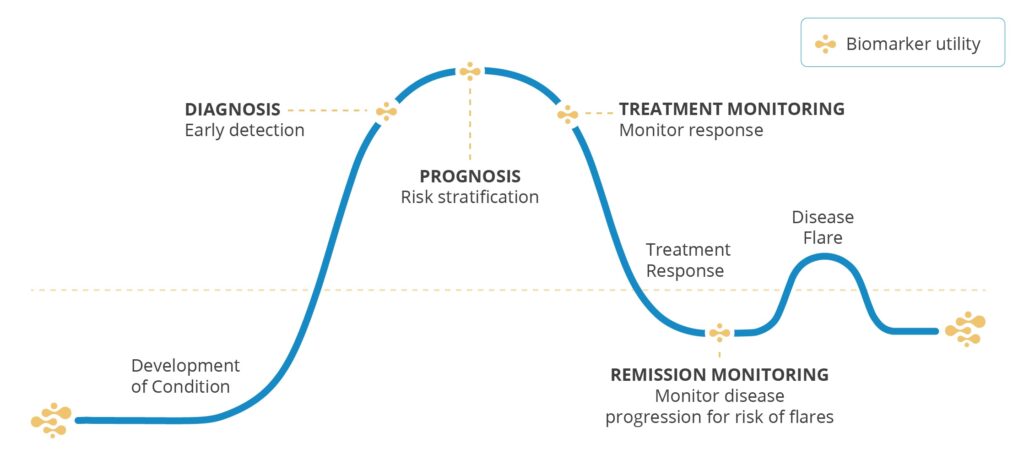
From data to decisions: the role of biomarkers in monitoring
RA management requires ongoing assessment—yet many standard-of-care biomarkers like RF and anti-CCP focus on static measures.
14-3-3eta is a joint-specific protein that fluctuates with disease progression and treatment response. Unlike traditional markers, it is modifiable and treatment-class agnostic, offering unique insights for RA monitoring.





Resources
References
- Coffey CM, Crowson CS, Myasoedova E, Matteson EL, Davis JM 3rd. Evidence of Diagnostic and Treatment Delay in Seronegative Rheumatoid Arthritis: Missing the Window of Opportunity. Mayo Clin Proc. 2019 Nov;94(11):2241-2248. doi: 10.1016/j.mayocp.2019.05.023. Epub 2019 Oct 13.
- Maksymowych WP, Naides SJ, Bykerk V, et al. Serum 14-3-3η is a novel marker that complements current serological measurements to enhance detection of patients with rheumatoid arthritis. J Rheumatol. 2014;41(11):2104-2113.
- Naides SJ, Marotta A. 14-3-3η in “Seronegative” Rheumatoid Arthritis. J Rheumatol. 2015;42(10):1995.
- Abdelhafiz D, Kilborn S, Bukhari M. The Role of 14-3-3 η as a Biomarker in Rheumatoid Arthritis. Rheumatol Immunol Res. 2021 Sep 28;2(2):87-90.
- Wijbrandts CA, Tak PP. Prediction of Response to Targeted Treatment in Rheumatoid Arthritis. Mayo Clin Proc. 2017;92(7):1129-1143. doi:10.1016/j.mayocp.2017.05.009
- Maksymowych WP, van der Heijde D, Allaart CF, et al. 14-3-3η is a novel mediator associated with the pathogenesis of rheumatoid arthritis and joint damage. Arthritis Res Ther. 2014;16(2).
- Carrier N, Marotta A, de Brum-Fernandes AJ, et al. Serum levels of 14-3-3η protein supplement C-reactive protein and rheumatoid arthritis-associated antibodies to predict clinical and radiographic outcomes in a prospective cohort of patients with recent-onset inflammatory polyarthritis. Arthritis Res Ther. 2016;18:3.
- Carrier N, de Brum-Fernandes AJ, Liang P, et al. Impending radiographic erosive progression over the following year in a cohort of consecutive patients with inflammatory polyarthritis: prediction by serum biomarkers. RMD Open. 2020;6(1):e001191.
- Hirata S, Marotta A, Gui Y, Hanami K, Tanaka Y. Serum 14-3-3η level is associated with severity and clinical outcomes of rheumatoid arthritis, and its pretreatment level is predictive of DAS28 remission with tocilizumab. Arthritis Res Ther. 2015;17:280.
- Orr CK, Najm A, Young F, et al. The Utility and Limitations of CRP, ESR and DAS28-CRP in Appraising Disease Activity in Rheumatoid Arthritis. Front Med (Lausanne). 2018;5:185. Published 2018 Aug 3. doi:10.3389/fmed.2018.00185
- Sornasse T, Chahal S, Gui Y, et al. AB0104: Correlation of plasma 14-3-3η levels with disease activity measures in methotrexate-naïve RA patients treated with upadacitinib monotherapy in the SELECT-EARLY phase 3 study. Annals of the Rheumatic Diseases. 2020;79:1351.
- Shovman O, Gilburd B, Watad A, et al. Decrease in 14-3-3η protein levels is correlated with improvement in disease activity in patients with rheumatoid arthritis treated with Tofacitinib. Pharmacol Res. 2019;141:623-626.
- Hirata S, Marotta A, Hanami K, et al. SAT0062: 14-3-3ETA predicts joint damage progression and flaring after adalimumab discontinuation. Annals of the Rheumatic Diseases. 2017;76:791.